Retatrutide: The Triple-Agonist Architecture Brief
Understanding GLP-1, GIP, and Glucagon Signaling in a Single Molecule
Executive Summary
Retatrutide combines three distinct signaling pathways within a single molecule — a structural design that represents the current frontier of incretin-based metabolic research.
- ✓GLP-1 Glucagon-Like Peptide-1 receptor agonism
- ✓GIP Glucose-Dependent Insulinotropic Polypeptide receptor agonism
- ✓Glucagon Glucagon receptor agonism
Unlike semaglutide (single agonist) and tirzepatide (dual agonist), retatrutide introduces a third pathway — glucagon receptor activation — intended to influence energy expenditure alongside appetite regulation and metabolic signaling.
The Evolution of GLP Signaling
Incretin-based research did not arrive at triple agonism in a single step. Each generation of compounds was built on evidence from the previous one. Understanding that lineage is understanding why retatrutide exists.
Semaglutide established that sustained GLP-1 receptor activation could produce meaningful metabolic effects at scale. That proof of concept raised the next question: could adding a second signal — GIP — extend those effects further? Tirzepatide answered that question with a substantial body of clinical evidence.
Tirzepatide's success with dual agonism then raised the question that retatrutide was designed to answer: what happens when glucagon receptor activation is added to the GLP-1 and GIP combination?
Each step was a deliberate architectural experiment, not an arbitrary escalation.
Researchers did not continue adding pathways because more is always better. They continued because each new pathway was hypothesized to contribute something the previous architecture could not — and evidence was the test of that hypothesis.
Understanding the Three Signals
Glucagon-Like Peptide-1
- Satiety signaling
- Gastric emptying
- Appetite reduction
- Glucose-dependent insulin secretion
Glucose-Dependent Insulinotropic Polypeptide
- Insulin regulation
- Metabolic support
- Synergistic signaling with GLP-1
- Nutrient-response activity
Glucagon Receptor
- Energy mobilization
- Metabolic activity
- Increased energy expenditure
- Hepatic glucose and lipid regulation
The addition of glucagon receptor agonism is what separates retatrutide from every previous generation. GLP-1 and GIP primarily address intake and signaling. Glucagon addresses the expenditure side of the metabolic equation.
Why Glucagon Matters
The Case for the Third Signal
For many people, glucagon is primarily associated with raising blood glucose levels. That framing is accurate but incomplete. Glucagon's role in energy management extends well beyond glucose counter-regulation.
At the systems level, glucagon is a mobilization signal. When the body needs to access stored energy — whether from glycogen in the liver or fat in adipose tissue — glucagon is part of the signaling cascade that initiates that process. It promotes lipolysis, increases hepatic glucose output, and contributes to thermogenic activity.
This is where the architectural logic of retatrutide becomes important. GLP-1 and GIP primarily act on the input side of the metabolic equation — reducing appetite, slowing gastric emptying, and modulating insulin response. Glucagon acts on the expenditure side — influencing how efficiently the body accesses and burns stored energy.
In a single-agonist or dual-agonist design, that expenditure pathway is not directly engaged. Retatrutide was designed to close that gap.
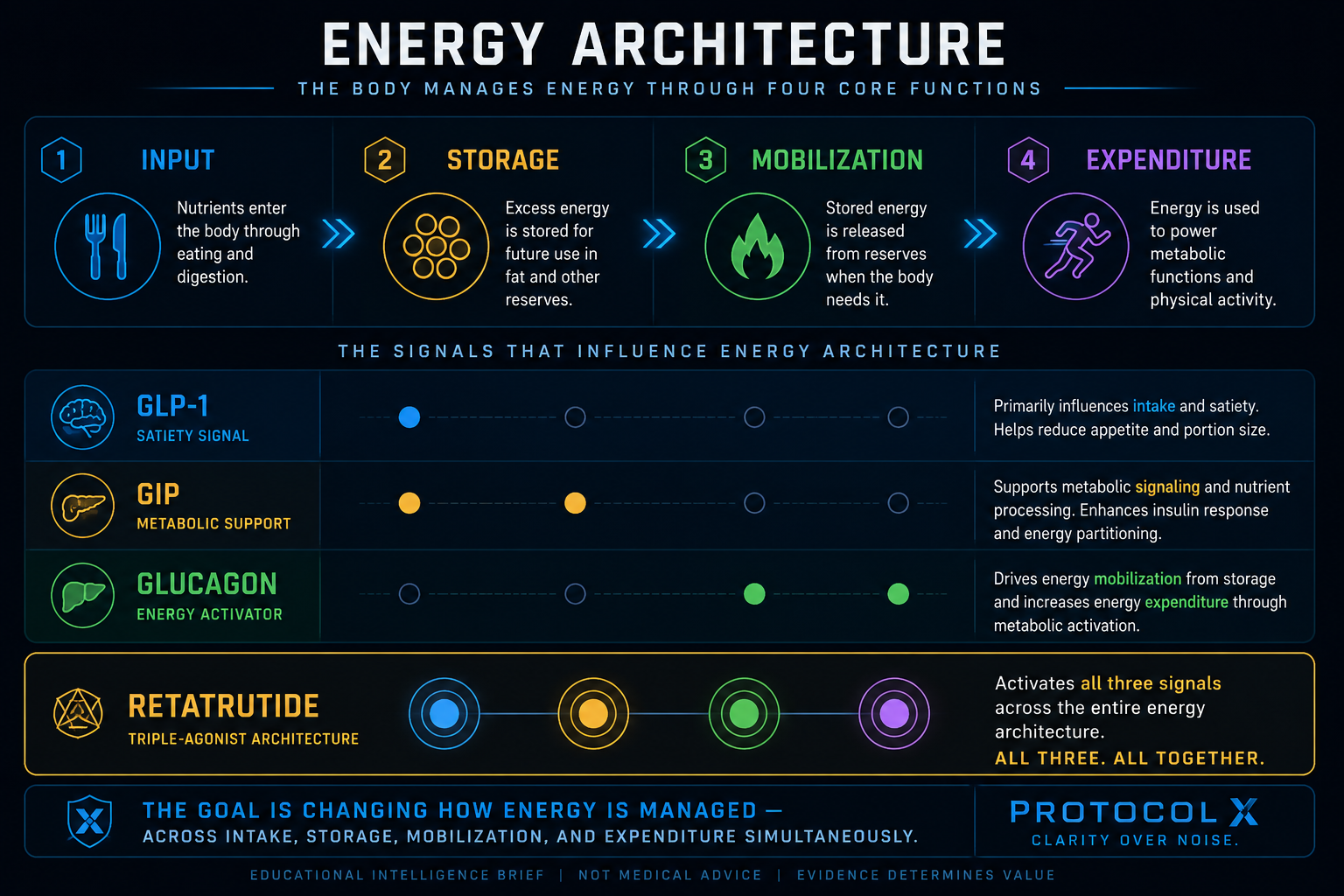
Energy Architecture Framework
GLP-1 primarily influences intake. GIP supports metabolic signaling. Glucagon contributes to mobilization and expenditure. Retatrutide combines all three pathways into a single signaling architecture.
The goal is not simply eating less.
The goal is changing how energy is managed — across intake, storage, mobilization, and expenditure simultaneously.
Potential Advantages of Triple Agonism
Research Areas Under Investigation
Retatrutide is currently under large-scale clinical investigation. The following represent areas where researchers are examining potential effects — not established conclusions.
- Weight management. Researchers are investigating whether triple agonism produces effects on body composition that are distinguishable from dual-agonist approaches.
- Metabolic health. The combined signaling architecture is being studied for effects across glucose regulation, insulin sensitivity, and related metabolic markers.
- Energy expenditure. Glucagon receptor activation introduces a pathway that may influence basal metabolic activity. Researchers are investigating the practical significance of this effect.
- Liver health. Glucagon has established roles in hepatic metabolism. Researchers are examining whether retatrutide's glucagon component produces measurable effects on liver-related markers.
- Cardiometabolic outcomes. As with previous incretin-based compounds, cardiovascular-adjacent outcomes are included in ongoing research programs.
Each of these areas represents an active research question, not a confirmed clinical outcome.
"Researchers are investigating" is not the same as "research has proven." These are hypotheses under active study — not clinical conclusions.
Challenges and Unknowns
What the Evidence Has Not Yet Answered
Retatrutide has generated significant early research interest. It has also generated a level of enthusiasm in popular media that runs considerably ahead of the available evidence. Protocol X treats that gap seriously.
- Longer-term data is still developing. Early-phase trial results are not the same as long-term outcome data. The durability of effects over multiple years has not been established.
- Tolerability considerations. Triple-pathway signaling creates a more complex pharmacological profile. Tolerability data, particularly at higher dose ranges, continues to be characterized.
- Complexity of triple-pathway signaling. Engaging three receptor systems simultaneously introduces interaction effects that are not always predictable from single- or dual-agonist data. The full picture of what three simultaneous signals produce — and in which populations — remains under study.
- Real-world durability remains under study. Clinical trial populations are controlled environments. How these findings translate across broader, more heterogeneous real-world populations is still an open question.
More signaling does not automatically mean better outcomes.
Architecture creates possibilities. Evidence determines value.
Retatrutide vs Semaglutide vs Tirzepatide
This is an architecture comparison, not a performance ranking. Each compound engages a different number of metabolic pathways. The question of which architecture produces the best outcomes for a given individual is a question only evidence — and clinical context — can answer.
| Compound | Architecture | Receptor Targets | Generation |
|---|---|---|---|
| Semaglutide | Single Agonist | GLP-1 | First Modern GLP-1 Agonist |
| Tirzepatide | Dual Agonist | GLP-1 GIP | First Dual Agonist |
| Retatrutide | Triple Agonist | GLP-1 GIP Glucagon | Triple Agonist Research Stage |
This is not a winner board. It is a map of how the architecture evolved — and why each layer was added. The value of each architecture depends on the evidence behind it, the individual using it, and the clinical context it is applied within.
Protocol X Assessment
- GLP-1 (Glucagon-Like Peptide-1)
- GIP (Glucose-Dependent Insulinotropic Polypeptide)
- Glucagon receptor agonism
Semaglutide showed what one signal could do. Tirzepatide showed what two signals could do. Retatrutide asks what three signals can do — and that question is still being answered.
The glucagon component is what makes this architecture distinct from everything that came before it. It extends the metabolic intervention from the input side — appetite and glucose regulation — toward the expenditure side, where stored energy is mobilized and burned.
Whether that extension produces clinically superior long-term outcomes at scale is the central open question. The early evidence is compelling enough to sustain large-scale investigation. The final answer requires more time and more data.
That is not a limitation of the compound. That is how evidence-based research works.